
The American Academy of Orthopedic Surgeons (AAOS) recently updated their practice guidelines for clinicians who treat patients with carpal tunnel syndrome (CTS). These guidelines were first introduced about 20 years ago. They have been revised to account for new information from up-to-date studies. Medicine is constantly evolving, with the goals of deepening our understanding of human diseases and improving the outcomes for our patients. Every few years the science is reexamined and updated as necessary to get closer to these goals. Continue reading for carpal tunnel syndrome updates.
The recommendations published by the AAOS are not meant to be a strict protocol; rather they serve as guidelines to consider in addition to the clinician’s independent medical judgement. These guidelines were developed by experts in their field after careful evaluation of the recent medical literature.
Detailed below are the most impactful practice guidelines for carpal tunnel syndrome, in my opinion. Please read the full set of AAOS practice guidelines for the complete list of recommendations.
Diagnosis is based on symptoms and physical examination
The diagnosis of carpal tunnel syndrome can be made based on symptoms and physical exam findings without the use of EMG (nerve conduction testing) or ultrasound examination. In other words, for most patients, additional testing is not necessary for a physician to proceed with treatment of carpal tunnel syndrome. Diagnostic ultrasound or nerve conduction testing may be obtained in specific patients who require additional clarification of the diagnosis. MRI imaging is not recommended for evaluating carpal tunnel syndrome.
Computers do not cause carpal tunnel syndrome
Computer keyboard use is not a risk factor for developing carpal tunnel syndrome. Despite what is a common belief in our society, there is insufficient evidence to conclude that computers cause CTS. This is an important carpal tunnel syndrome update.
Steroid injections are available for temporary relief
Corticosteroid injections may provide short term relief of patient symptoms, but do not provide long term improvement of carpal tunnel syndrome. Corticosteroid injections are low cost, very common, and popular treatments for CTS. They can be used for short term relief of symptoms as well as aid in the diagnosis of carpal tunnel syndrome.
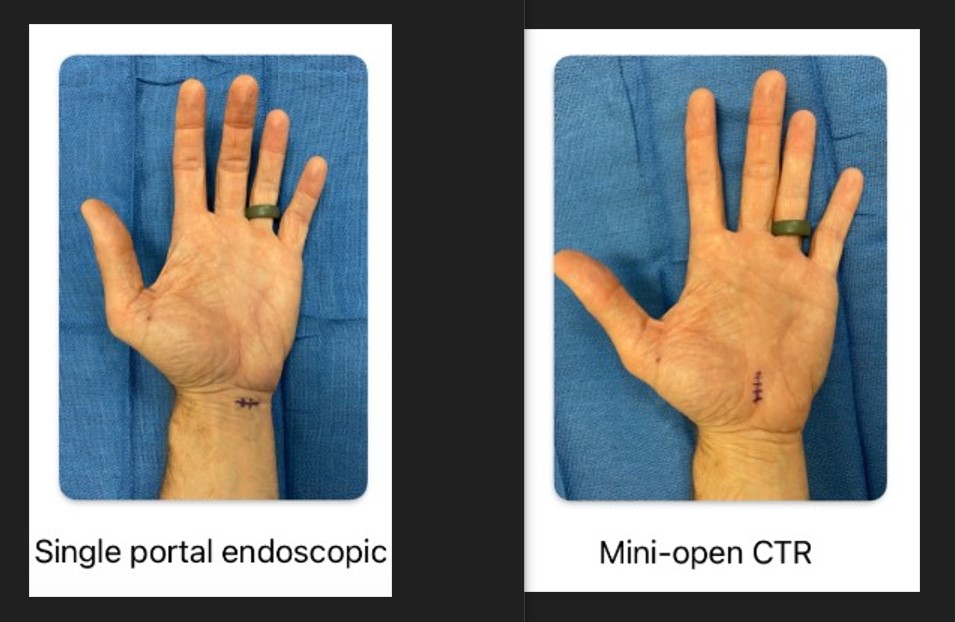
Mini Open and Endoscopic Surgery are Options
Mini-open and endoscopic carpal tunnel release surgeries are both accepted surgical options for treatment of patients with carpal tunnel syndrome. The AAOS committee does not consider one technique to be better than the other. There are advantages and disadvantages to either surgical option, which may be considered by the treating surgeon.
Therapy is not required after surgery
In general, physical therapy or occupational therapy is not recommended in routine postoperative carpal tunnel release cases. Therapy may be beneficial in some patients as determined on a case-by-case basis.
Use of a wrist splint and/or sling are not recommended after carpal tunnel surgery. Prolonged immobilization can result in stiffness and delayed recovery from this type of surgery.
Ibuprofen and Tylenol are recommended after surgery
Ibuprofen (Motrin) and/or Acetaminophen (Tylenol) are recommended medications for pain management following carpal tunnel release surgery. The committee recognizes the potential adverse effects of opioids, including side effects, overdose, and addiction. Therefore non opioid medications should be used when possible. These common medications are purchased over-the-counter at a low cost.
If an opioid medication is prescribed after carpal tunnel surgery, tramadol may be considered instead of other opioids. Tramadol is considered to have less potential for side-effects, overdose, and addiction compared to other opioids.
Surgery does not require hospitalization or general anesthesia
Carpal tunnel surgery can be safely performed in the office setting with local anesthesia only, limited surgical draping, and without routine preoperative testing (blood tests, chest x-ray, and EKG). Most patients do not require treatment in the hospital operating room, which can therefore provide cost savings for patients.
Antibiotics are not necessary
Antibiotics are not recommended in the setting of carpal tunnel release surgery. The risk of surgical site infection is very low after carpal tunnel surgery, and prophylactic antibiotics have not been shown to reduce this risk.
Many available treatments are not effective
There are many treatments available for patients with carpal tunnel syndrome which have not shown to be effective in scientific studies. These treatments include: acupressure, magnet therapy, phonophoresis, oral NSAIDs, nutritional supplements, heat therapy, and platelet rich plasma injections (PRP). These treatments are not cost-effective or recommended by the AAOS committee.
Other treatments which do not provide long-term improvement for patients with carpal tunnel syndrome include: oral steroids, laser therapy, shockwave therapy, massage therapy, hydrodissection, kinesiotaping, therapeutic ultrasound, and manual therapy. It is possible that these treatments provide short term symptom relief for patients. However, these treatments are not cost-effective or recommended by the AAOS committee.
Updated by Dr. John Erickson on 1/7/2025.
Disclaimer: Please note, the material provided on this site is intended for general information only and does not constitute medical advice. This does not replace evaluation by a doctor. Please seek medical evaluation if you have a concern.